
Surgical Section
The information on this page is intended for health professionals reference and use only. If you are a parent or family member looking for information about treatment, please visit unit information.
Contents
1.0 Aim of guideline
2.0 Scope of guideline
3.0 Guideline summary
4.0 Guideline Framework
4.1 Background Information
4.2 General Care Principles
4.3 Skin Care Products
4.4 Irritant Contact Dermatitis (nappy rash)
4.5 Use of Adhesive Products
4.6 Dry Skin
4.7 Pressure Area Care
4.8 Handling Infants on the Neonatal Unit
4.9 Documentation and Photography
4.10 Staff
4.11 Parents
4.12 Audit
5.0 Glossary of Terms
6.0 Guidelines for Bathing Infants on the Neonatal Unit
6.1 Who Can be Bathed?
6.2 Best Skin Care Practices for Term Infants (37 weeks gestation upwards)
6.3 Preterm Infants (less than 37 weeks gestation)
6.4 General Skin Care
6.5 Outcomes of Bathing Infants Less Frequently
6.6 First Bath
6.7 General Guidelines
6.8 Safety
6.9 Parents
6.10 Swaddled Bathing
6.20 Additional Bathing References
Appendices
Appendix 1 – Example of a blank body map, that can be used to document specific location of areas of skin damage or concern for the hospitalised neonate
Appendix 2 – Example Skin Map of the body used by Milton Keynes General Hospital Neonatal Unit
Version Control
1.0 Aim of Guideline Framework
This guideline has been produced to direct staff in their care of neonate’s skin. The guideline is based on research findings and/or currently accepted best practice. For accessibility, the guidelines have been collated under distinct subheadings. However, the reader is advised to read the guidelines in full and to seek the advice and support of more senior or experienced colleagues, in the practice setting.
For guidance on the issues listed below please see separate TVWNODN guidelines available at https://neonatalnetworkssoutheast.nhs.uk/professionals/guidelines/tvw-guidelines/
2.0 Scope of Guideline Framework
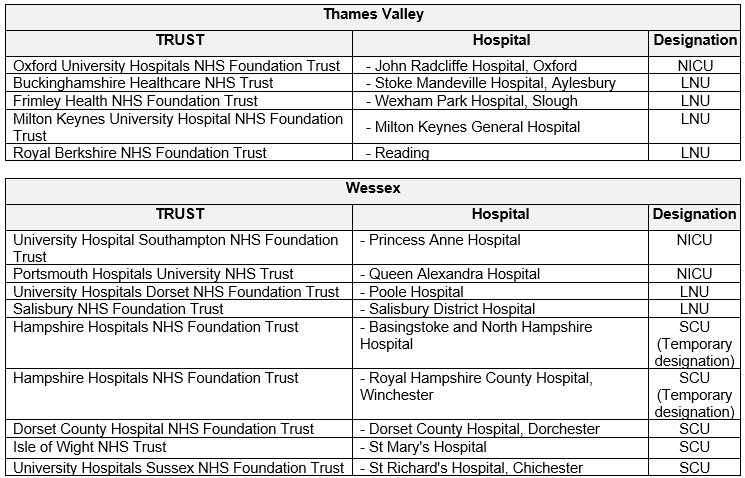
The guideline applies to all Neonatal Units and Maternity Units covered by Thames Valley & Wessex Neonatal ODN. This includes the following hospitals:
3.0 Guideline Summary
Assessment and documentation
- Assess the infant’s skin condition on admission and at the commencement of each shift and document findings in a designated place, i.e. Nursing care plan, Medical notes/ record, or Skin Integrity Care Plan).
- Note and record in the designated place any; bruising, significant reddening/purple colouration, broken skin, swelling or demarcated changes in colour or texture.
- If skin damage is identified there should be immediate action taken to see if the cause of the damage can be identified, and further damage prevented.
Best practice principles
- At least once per shift observe and clean areas of skin that are vulnerable such as the neck, behind the ears, axillae and groin.
- Use plain water for skin cleansing and pat skin dry instead of rubbing dry.
- Vernix caseosa should be left on the skin of all newborn infants to absorb naturally.
- If any changes are made to the skin care regime of an infant, then the new regime should be tried for at least 24 hours, before making a decision about its effectiveness.
- All probes/ monitoring equipment should be regularly repositioned to minimise the risk of pressure.
- Great care should be taken to ensure that babies are not positioned so that they are lying on tubing, IV fluid lines, nasogastric tubes etc.
- The use of adhesive tape should be kept to the absolute minimum and a pectin based barrier should be placed underneath adhesive tape for skin protection.
- Use a liquid barrier film to protect the skin, before applying an adhesive device to the skin, i.e. stoma bag.
- To remove adhesive utilise an adhesive removal product (i.e. Appeel).
- ECG electrodes should be of the Hydrogel type.
- Visibly dry skin on a neonate should be left to recover and repair itself. Do not apply moisturising products.
Products
- Any product used on neonatal skin should be; licensed for use on babies, single patient use only, pharmaceutical grade and where possible sterile before opening.
- Never use Peanut oil (arachis oil), Alcohol, or acetone plaster remover.
Irritant contact dermatitis (ICD)
- If an infant has ICD contact dermatitis (nappy rash) their skin should be cleansed as soon as possible after nappy is soiled.
- Four different practices can be used to try and combat ICD, these being; Applying a barrier preparation, Using liquid barrier film, Using an emollient cleaning additive, Exposing skin to air.
- Persistent and non-responsive nappy rash should be swabbed, but anti-fungal or anti-bacterial creams should only be used for strongly suspected or confirmed infection.
High risk Infants
- Infants most at risk of pressure related skin damage are; the extreme preterm, those with restricted movement, critically ill infants, or infants nursed on the firmer surface of a fibre optic phototherapy ‘blanket’, nursed on nasal prong/ nasal mask CPAP/ DUOPAP or needing regular handling for blood tests, lumbar punctures etc.
- For these infants aim to do regular repositioning, consider pressure relieving mattress, extra vigilance of skin integrity, handle with care, monitor high risk sites such as ears and bony prominences.
Bathing
- Bath infants in plain water, for a maximum duration of 5 minutes. If the umbilical cord remains in situ use shallow water and do not soak the cord stump. Frequent bathing is not advised.
4.0 Guideline Framework
4.1 Background Information
The skin is a vital organ with many roles and functions. These include thermoregulation, provision of a barrier against toxins and infections, water and electrolyte excretion, fat storage and insulation, and tactile sensation. Preserving the integrity of skin is an important aspect of nursing care, across the lifespan for all patients, but is of particular significance in newborns who are adapting from the uterine aquatic environment to the aerobic environment. (Lund et al 1999)
In addition, the skin of a premature infant is not fully developed and has many unique physiological and anatomical factors that make their skin very vulnerable to damage. These include; limited subcutaneous fat, oedema, immaturity of the skin capillary network, underdevelopment of the stratum corneum and diminished cohesion between the epidermis and dermis. (Marcellus, 2004)
Maintaining skin integrity for neonates within the Neonatal Unit is a challenge for staff due to care practices such as bathing, lubrication, antimicrobial skin disinfection, adhesive removal and frequent handling (Lund, 1999). In addition, skin care practices used and recommended within different Neonatal Units has been found to vary significantly, causing confusion for staff and parents and inconsistent care for infants. (Jackson, 2008. Nurse.com, 2001)
It is accepted in the literature that optimizing skin care for infants by creating and applying evidence based skin care practices can improve patient outcome and may reduce long term costs and morbidity in this group. (Furdon 2003. Munson et al 1999) It is with this background that the guideline is written.
4.2 General Care Principles
- Assess the infant’s skin condition on admission and at the commencement of each shift (or first suitable opportunity – bearing in mind baby’s behavioural cues and sleep/wake state). Document findings in a designated place.
- Staff should be proactive, and if the infant is stable enough at least once per shift observe and clean areas of skin that are vulnerable such as the neck, behind the ears, axillae and groin.
- Staff should be observant for any skin that is dry, red, and itchy or has lesion (pustular, vesicular or purulent) – as skin integrity may be impaired and early action may be taken to prevent further compromise.
- Staff should note – and report to the medical team or senior nursing colleague;
- Bruising.
- Significant reddening/purple colouration.
- Broken skin.
- Swelling.
- Demarcated changes in colour or texture.
- Specific shape or type of damage caused by equipment – i.e. red circles from TCM, SaO2 probe, ECG leads, pressure damage from lines or cables.
- There should be immediate action taken to see if the cause of the damage can be identified, and further damage prevented.
- Plain water should be the first choice for skin cleansing.
- Carers should pat skin dry after cleansing, instead of rubbing dry.
- Vernix caseosa should be left on the skin of all newborn infants to absorb naturally.
- If an infant is born with skin contaminated by meconium or blood, staff should not rush to remove it just to make the baby ‘look clean’. It can be left many days if necessary (i.e. in the extremely ill baby) before cleaning.
- If any changes are made to the skin care regime of an infant, then the new regime should be tried for at least 24 hours, before making a decision about its effectiveness.
- Probes may compromise the infant’s skin by causing pressure necrosis. This can occur, especially if the infant is extremely preterm, where the dermis is oedematous and this reduces blood flow to epidermis and makes the skin more susceptible to breakdown. All probes/ monitoring equipment should therefore be regularly repositioned to minimise this risk.
- ECG leads can usually be left in place.
- Saturation probes tend to compress the foot, hand or ankle and should be moved after 4 to 6 hours, or more frequently if the baby’s skin is marking. Avoid overtightening the fixation.
- Temperature probes can cause indentation of the skin and need to be moved every 4-6 hourly. Staff should ensure that babies are not laid on the temperature probe, as this will exacerbate skin compromise.
- Blood pressure cuffs ‘squash’ the skin, as well as sometimes digging in to the skin on their upper or lower edges and should be relocated every 4-6 hours, more often if the cuff is being inflated very frequently.
- Beware when siting probes, that they are not overlaying or unintentionally fixed to any wound or wound dressing. This could cause pain, or affect the integrity of the dressing, increasing the risk of infection or wound breakdown.
- When performing heel pricks on neonates for blood sampling, never use an improvised warming device, such as a glove filled with hot water to warm the infant’s foot. There is a significant risk of scalding or burning the infant’s foot/skin directly through the glove. The heated item can also burst and spill its hot contents onto the infant.
- If the infant’s perfusion is poor, it may be possible instead to improve this prior to blood sampling, by putting socks/ knitted booties onto the baby’s feet. Or by utilising a single use, safety checked, medical grade foot warmer- designed for the purpose.
4.3 Skin Care Products
- Wherever possible any product used on an infant’s skin should be licensed for use on neonates.
- Any product applied to an infant’s skin should be single patient use only.
- Any product applied to the infant’s skin should be pharmaceutical grade and where possible sterile before opening.
- When using skin care products, care must be taken to avoid contaminating the contents of a container. The required amount should be poured or spooned into an appropriate pot, or hands decontaminated and a clean glove applied between touching the baby and putting product onto the fingertips for application.
- Products applied using an impregnated wipe should be dabbed onto the skin, not rubbed on vigorously.
- Products designed to be applied by spraying must not be used in incubators – due to the risk of inhalation. Carers must either remove the infant briefly from the incubator whilst spraying occurs or spray the products onto gauze (or similar) and then transfer the product to the infant’s skin.
- The decision to use products with a strong smell should be balanced with the risks of over stimulation or even damage to the olfactory system.
- Some products or ingredients have a particularly high risk of causing sensitivity, allergy or anaphylaxis and should be avoided completely. These include;
- Peanut oil (also known as arachis oil).
- Alcohol.
- Plaster remover (traditional acetone based type).
- Carers should be aware that an infant’s skin may be very slippery after application of certain products – extra care may be needed when handling the infant.
- Carers should be aware that infants requiring phototherapy will be limited in the products that can be applied to their skin – due to the risk of burning when oily skin is exposed to the ultra violet lights. See phototherapy guideline for further information.
- If parents/ families wish to use baby wipes after their baby is term, they should be alcohol free.
- There is disagreement within the literature about the benefits, or otherwise of using topical emollient therapy for neonatal skin. Researchers have identified that regular application of emollients helps to improve the skin integrity of premature babies. However, some studies have identified an increased risk of serious infections- particularly coagulase-negative staphylococcus (CoNS) and candida.
- There appears to be some variation, between the outcomes of studies carried out in the developing and developed world, perhaps related to the extremity of prematurity of the infants who participated in the studies. However, the overall current opinion is that topical petroleum ointment may increase infection and shows no strong evidence of significant benefit, such as reduction in invasive infection or death. Therefore, the practice of applying topical emollient routinely, to a preterm infant’s skin cannot be recommended.
4.4 Irritant Contact Dermatitis (nappy rash)
- Categories of infants found at particular risk include those;
- On IV antibiotics (altered intestinal flora).
- Neonatal abstinence syndrome.
- On preterm formula.
- Recent changes in diet, i.e. from breast milk to formula.
- Babies on minimal handling regimes.
- Infants who are teething.
- Skin products should not be used routinely when no problem is present. In particular antiseptics are not needed as bacterial infection is not the cause of nappy rash.
- Treatment should focus upon protecting the damaged skin and reducing friction to reddened or sore area.
- Carers should clean nappy area gently and never ‘scrub’ at skin.
- Skin should be cleansed as soon as possible after nappy is soiled (balanced with need for rest/minimal handling).
- Consider four options;
| Applying a barrier preparation. | See glossary in section 5.0 or on pages 15 – 18 of PDF guideline for further details |
| Using liquid barrier film. | |
| Using an emollient cleaning additive. | |
| Exposing skin to air. |
- Persistent and non-responsive nappy rash should be swabbed for fungal and bacterial infections, as nappy rash can be secondary colonised.
- Anti fungal or anti bacterial creams should only be used for suspected or confirmed fungal (mostly candida) or bacterial infection.
- Corticosteroids should only be used when all other treatments have failed and for no more than a week.
4.5 Use of Adhesive Products
- The use of adhesive tape should be kept to the absolute minimum.
- A pectin based barrier should be placed underneath adhesive tape for skin protection.
- When removing adhesive tape/products from the skin ease the product off gently using one of the three listed processes:
- Moisten with water and cotton wool and ease off gently.
- Moisten with water with an emollient cleansing additive and ease off gently.
- Utilise an adhesive removal product (i.e. Appeel) designed for use on human skin. These products are silicone based and latex free and come in three preparations; a liquid, spray or as an impregnated wipe. The manufacturer’s instructions should be followed for using each type of preparation.
- Neonatal Units are reporting that the liquid preparation is particularly effective in removal of dressings, stoma bags and endo-tracheal tube fixations systems which adhere to the face. Where previously these procedures caused pain and skin trauma, staff are reporting pain free and trauma free adhesive removal.
- Removing adhesive products is a potentially painful procedure- use of oral sucrose and/or non-nutritive-sucking should be considered.
- Any adhesive device used to secure nasal cannulae must be designed for the purpose and for neonatal use.
- Any adhesive device used to secure an ET tube must be designed for the purpose and for neonatal use.
- Consider using a liquid barrier film to protect the skin, before applying an adhesive device to the face, such as to secure an ET tube.
- Where tape must be placed against the skin of term infants – such as for securing an iv splint to a vigorous infant, consider using tape that is easily removed by an adhesive removal liquid preparation. For example, absorbent tape varieties such as ‘Elastoplast’ or ‘Mefix’. This choice of method can be an effective way of safely using tape on the term infant, without damaging the infant’s skin, and minimising distress to the infant.
- For securing peripheral venous lines an adhesive product will need to be applied directly onto the skin. However, it must be sterile and designed both for the purpose and for neonatal use.
- For securing central venous lines an adhesive product will need to be applied directly onto the skin. However, it must be sterile and designed both for the purpose and for neonatal use.
- Non adhesive wraps should be used to hold a saturation probe in place.
- ECG electrodes should be of the Hydrogel type.
- To remove Hydrogel ECG leads saturate the hydrogel using water (by spraying, on a cloth, or immersion in a bath) before peeling off gently.
- Refer to photographs below, for how to correctly remove transparent film dressings (such as Opsite, Bioclusive or Tegaderm)
4.6 Dry Skin
- Visibly dry skin on a neonate should be left to recover and repair itself. Do not apply moisturising products which only alter the cosmetic appearance of the outer skin layers.
- Recent research (OBSeRvE, 2015) has shown that whilst the preterm infant’s skin treated with oil is hydrated due to glycerol in the oil staying on the skin, the fatty acids in the oil penetrated the skin and adversely affected the skin barrier (this effect cannot be seen by eye).
- If the dry skin is felt to be so severe it is causing an infection risk, then emollient or similar products should only be applied under medical direction and with a prescription.
4.7 Pressure Area Care
- Infants have a large surface area to weight ratio, so pressure injuries are not that common in Neonates. However, research has shown that infants most at risk of pressure related skin damage are those;
- Extreme preterm infants 26 weeks and below.
- Infants with restricted movement (i.e. pharmacological paralysis, movement disorders, hydrocephalus or spina bifida).
- Critically ill infants, with possible poor tissue perfusion, poor nutrition, oedema and restricted movement.
- Infants nursed on the firmer surface of a fibre optic phototherapy ‘blanket’. Extra vigilance should be taken when caring for and handling such infants, both to prevent pressure and to monitor sites of high risk. Such sites include bony prominences such as;
- Knees.
- Elbows.
- Ankles.
- Pelvis/hip bones.
- Shoulders if laid laterally.
- Scalp.
- Hydrocolloid dressings have been found to be effective protection against pressure on skin that is showing the early signs of chaffing. For example on knees or elbows that have become red when an infant is nursed prone. (Taquino 2000)
- There are many products on the market for reducing pressure of the neonatal bed surface. For example; gel mattresses, gel pillows, synthetic sheepskin fabric, homemade fabric and wadding pads, air mattresses, memory foam mattresses. There has not been comprehensive testing or comparison of different products, to be confident which if any are effective. However, it seems logical that the softer more yielding surface would offer some benefit to the at risk neonate. In addition any products used should be designed for the purpose of neonatal positioning, be safety checked and able to be washed at 60 degree centigrade or cleaned according to local infection control policy.
- Regular repositioning can help relieve and redistribute pressure on an infant’s skin, but must be balanced with the need for sleep and fragility of the infant. See the SCNN supportive positioning guideline for further advice in this area.
- Great care should be taken to ensure that infants are not positioned so that they are lying on tubing, IV fluid lines, nasogastric tubes etc.
- Staff should be aware that an infant’s ears are vulnerable to pressure injury because of their cartilaginous nature and because infants can often be laid on their ears for prolonged periods of time. Be particularly aware of any nasogastric tube that is secured so that it passes across an infant’s ears, as a purple ‘line’ of pressure sore can develop underneath it.
- For infants nursed on nasal CPAP or nasal High Flow Therapy (nHFT) there can be pressure on the skin of the nares due to the nasal prongs. The prongs should be briefly removed with every episode of care, to inspect for injury, relieve pressure and change the position, even slightly. For more in depth information see relevant CPAP and nHFT nursing care guidelines.
4.8 Handling Infants on the Neonatal Unit
- Staff should take particular care when a procedure requires some pressure to be exerted on the infant’s skin. For example heel-prick blood sampling, restraining for a lumbar puncture, siting a central line. Bruising, shearing trauma and petechial marking can all occur very easily, especially in the extremely premature infant less than 26 weeks gestation.
- All new staff should be supervised by an experienced colleague, until competent, when learning to take blood specimens from infants. Formal assessment of competence should occur.
4.9 Documentation and Photography
- There should be daily documentation of skin integrity, in a record that will be retained – such as nursing evaluation or medical notes.
- Documentation should include the skin’s condition and where relevant, any actions or treatment regimes in progress and their effect.
- Where possible photograph(s) should be taken of significant skin damage, breakdown or injury and placed in medical record for reference. Taking and storage of photographs must comply with local policy on consent and information governance. Medical photography can be contacted to do this but may not be available all of the days or times when images are required.
- With recent technological advances, if the local trusts rules allow this, staff can use an app such as ‘Clinical Uploader Pro’ to take the photograph on their camera phone. The app enables these images to move electronically and directly into the infant’s medical record, and clinical images are never stored on the individual’s actual camera phone.
4.10 Staff
- Staff should follow the clinical guidelines and protocols in places on their neonatal unit relating to maintaining skin integrity.
- Staff who are seeking further information and/or support should refer to:
- The nurse in charge/ clinical development nurse.
- Tissues viability/wound care consultant.
- The Unit wound care link nurse.
- Unit training/orientation packages on maintaining skin integrity.
- Electronic resources on the hospital tissue viability website.
- Journal articles relevant to neonatal skin integrity.
- Manufacturer’s guidelines for particular products.
- The children’s BNF.
4.11 Parents
- Parents should be involved and informed about their baby’s care, including about infant skin care and how we work together to maintain and promote the skin integrity of preterm and unwell infants. This may include through conversation, and also by offering access to written, online and other resources on this topic.
- Parents should be offered explanations for why using toiletry products on their baby’s skin may be unsuitable at this time. Explanations should include information about the preterm infant’s developing, but vulnerable skin, and the reasons for avoid some products, or delaying their use until the infant has a more mature skin barrier.
- Parents should be involved in decision making about their baby’s skin or skin care whenever appropriate. This should include keeping them informed of changes in their baby’s skin condition and any current treatment and/or prevention regimes they are requiring.
- Open and honest communication should be maintained between Neonatal Unit staff and parents. If a specific incident or event occurs to damage an infant’s skin, parents should be informed of the episode, its cause and any proposed or actual treatment, as soon as practically possible. When parents have been informed, this should be documented, or if there is a delay in informing parents, the reasons for any delay should be recorded.
4.12 Audit
- All staff should assist with and participate in audit that is being carried out with respect to the neonatal skin integrity.
5.0 Glossary of Terms
Barrier Preparations
They try to mimic the stratum corneum by forming a durable, long lasting protective barrier that maintains optimum moisture levels (Atherton and Mills, 2004) They should ideally be fragrance free, preservative free, allow skin to breathe, easy to remove, antiseptic free and with proven clinical efficacy. Careful attention should be paid to their instructions for use.
- Bepanthen – the only barrier preparation shown in trials to both prevent and treat nappy rash including preterm infants (see Putet et al, 2001).
- Metanium – apply thinly so skin can be seen through ointment. Clean skin before reapplication, but all traces of cream do NOT have to be removed. For very sore skin, vegetable oil can be used in place of water to clean skin and remove previous layer of Metanium with minimum abrasion.
- Sudocrem – contains antiseptic and fragrance which are not necessary.
- Zinc and castor oil ointment – contains arachis oil and should not be used.
- Medical grade honey, barrier cream – products with honey in are becoming widely used in neonates. Can be applied to intact skin and has natural antiseptic properties. Refer to manufacturer’s instructions for use as varies between each product.
Emollient cleaning additives – (i.e. Oilatum, Balneum, E45 bath oil)
These products can be added to the water used to clean an infant’s nappy area or applied directly to the skin and rinsed off. They hydrate the skin and leave an oily film on the skin which provides a barrier to moisture and can help reduce friction. In some Units an infant with nappy rash will not have their skin wiped clean, but instead rinsed/washed with such a product in a bowl of water.
Exposing sore skin when a baby has irritant contact dermatitis
Allows the skin to dry and prevents urine from sitting in contact with the skin. Friction to the skin is minimalised and carers are able to see and act as soon as the nappy area has been soiled.
- Remove nappy and clothing from legs and lower body, so that sore nappy area is in contact with air.
- Nurse the infant on an absorbent disposable pad, or if nursed prone the infant can be laid on nappy, but with nappy flapped open so area around anus is dry and exposed. Cot covers will only be covering the infant’s upper body.
- Monitor the baby’s temperature closely. Carers may need to move the infant to an incubator, give the infant extra clothing, or some Units will place a domed plastic shield over the infant’s lower body, and then place bedding over this.
- The infant should be closely observed, and the nappy area cleansed as soon as soiling is noted.
- Some infants tolerate exposing less well than others. If this is so, consider exposing a baby only between alternate feeds. Or just over night, when there may be less disturbance.
Liquid barrier films (LBF) i.e. Cavillon
Generally a silicone-based fluid that evaporates from the skin leaving behind a clear waterproof layer over the surface of the skin. Comes in the form of a wipe, spray or coated swab, promoted as non-irritant, alcohol free and waterproof. Frequency of application typically 24 – 48 hourly, as film layer persists. Not licensed for neonates but widely used in Neonatal Units without reports of adverse effects.
LBF’s can be used as a skin protectant for infants with vulnerable skin, for example under clear IV dressings or facial oxygen cannulas. This is best done using a light spray or using a wipe or swab.
- The area to be ‘coated’ must be clean and dry.
- If spray is to be used, the surrounding areas must be covered, to prevent inadvertent contact with the spray.
- The LBF should be left for 30 seconds to dry completely.
LBF’s can also be used as a treatment for sore bottoms.
- Clean the nappy area with plain water.
- Using the coated swab, apply a thick coat of LBF all over the affected area- including all raw and bleeding areas.
- Leave to dry for 30 seconds before applying nappy. Ensure that any LBF in skin folds does not stick to the opposing skin fold.
- On subsequent nappy changes clean area with plain water and cotton wool, do not try to remove the LBF. The LBF may become discoloured or start to peel – do not worry about this.
- Apply a new layer as directed, usually 48 hourly to start with, but can be applied more frequently if required.
- Do not apply LBF to the peri-anal area on female infants as the urethra could be accidentally covered.
Topical ointment
The prophylactic application of topical ointment to preterm skin has previously been suggested as a method for seeking to maintain its barrier function. However, a recent Cochrane review of this practice has concluded that this practice increases the risk of coagulase negative staphylococcal (CONS) infection and should NOT be used routinely in preterm infants.
Skin Map
Consider using a skin map of the infant, which can be annotated to document areas of damaged or broken skin.
See appendix 1 and 2, on pages 23 and page 24, for an example
Vegetable Oils
Oil has generally been used in two ways on the skin of infants;
Firstly as a skin ‘conditioner’ applied generally to large areas of an infant’s skin to improve its appearance. This practice is not encouraged as neonates skin should be allowed to hydrate and heal naturally as there is felt to be only a cosmetic benefit from its application. Also applying oil increases the risk of nosocomial infections. If a parent is persistent that they wish to use oil, it should only be applied to stable infants who are post term and with consideration of the guidelines below.
Secondly, oil is used as an alternative to water, to clean the nappy area for infants with contact dermatitis. It has been found useful for gently removing skin barrier products such as Metanium without any need to rub the skin surface. However, there is great inconsistency in the literature about which oils are most effective and have least complications.
Some useful principles used by other Neonatal Units;
-
- Refined oil should be used due to its limited smell, thin texture, longer shelf life and reduced likelihood of containing impurities such as yeasts, moulds, or fungal spores.
- Do not use mineral (paraffin) oil as it leaves a greasy layer on the baby’s skin which may seal up the pores.
- Do not use products containing essential oils, as the smell could overwhelm neonates’ sensitive physiological system.
- Avoid nut oils as they have the potential to cause sensitisation/ allergy.
- Avoid placing oil onto broken areas of skin, as the risk of allergen exposure is elevated in this situation.
- Sunflower oil is considered a good selection for use on infants. It is high in Linoleic acid which mirrors skin lipids and has regenerative, restructuring and moisturising properties. A supply of refined, deodorised and heat treated oil is available from Huddersfield Royal Infirmary Hospital Pharmacy.
- Fractionated coconut oil is also considered a good selection for use on infants (the fractionation process removes most of the proteins that may attach to allergens).
- Olive oil should not be used as it is high in oleic acid which can damage the stratum corneum. It is also not advisable due to its stickiness and strong odour and possible contamination with bacteria and fungus- if a cold pressed non-sterile supply is used.
- Peanut- (arachis oil) must not be used due to its elevated risks of allergic or anaphylactic response.
6.0 Guidelines for Bathing Infants on the Neonatal Unit
6.1 Who can be bathed?
- Only infants large enough and well enough to be nursed in cots should be bathed.
- The infant should have been physiologically stable for at least 48 hours.
- The infant should have been thermally stable for at least 48 hours.
6.2 Best Skin Care Practices for Term Infants (37 weeks gestation upwards).
- Bathing frequency should be a maximum of 2-3 times a week.
- Plain water should be used for the first 2-4 weeks. If parents then wish to use toiletry products, introduce them gradually.
- Bath should be a maximum of five minutes duration.
6.3 Preterm Infants (less than 37 week’s gestation)
- Bathing frequency a maximum of every 3-4 days.
- Preterm infants should only be bathed in plain water.
- If toiletry products are introduced when an infant’s corrected gestation is 37 weeks, they should be introduced gradually over 2-4 weeks.
- Bath should be a maximum of five minutes duration.
6.4 General Skin Care
- The use of toiletry products at any time should be actively discouraged by staff.
- If a parent wishes to use toiletry products after the 2-4 week period of plain water bathing, then the products should ideally be;
- Manufactured for newborn infants.
- Perfume free.
- Colour free.
- Not alkaline in nature.
- Hydrogel ECG leads do not need to be removed from an infant’s skin for bathing. The moisture will usually help to rehydrate the gel and assist in their continued adhesion. (For safety, the leads should be disconnected from the monitoring equipment before immersion.)
- When drying an infant after its bath, do not rub the skin to dry it, instead pat skin gently with towel.
6.5 Outcomes of Bathing Infants less frequently
| Outcomes of bathing neonates less frequently |
| Less physiological stress |
| Less behavioural stress |
| Skin flora colonisation not effected |
| Skin pathogen colonisation not effected |
| Less drying and irritation of skin |
| Acid mantle is able to mature |
| Reduced exposure to chemicals in toiletry products, that may be absorbed into skin |
6.6 First Bath
- A baby’s first bath is an important family event and should whenever possible be performed with parents present.
- If parents cannot be present for a first bath, then staff must ensure parents are aware it will be done without them and that parents have consented to this.
- Remind parents to bring in a camera for taking photographs of a baby’s first bath. Consider taking a photograph for parents who are not able to be present.
6.7 General Guidelines
- The vessel in which the infant is bathed should have been designed for the purpose of bathing infants.
- Test water temperature before placing infant into the water, using technique dictated by local policy.
- Bath water temperature should not exceed 37degrees centigrade.
- The room should be warm and draught free.
- If an infant still has their umbilical cord stump in situ, the water should be shallow enough that the cord stump is not continuously submerged.
- If the infant has no umbilical cord stump in situ, then the depth of water can be based on the parents and baby’s preferences.
- Baths are generally best carried out before an infant is fed. The infant is more likely to be awake and alert and less likely to vomit than after a feed.
6.8 Safety
- Parents should be supervised when bathing their infant until deemed to be competent.
- Staff should follow manual handling guidelines when moving a bath that may be heavy, awkwardly shaped and difficult to balance.
- If possible do not move the baby bath when full of water. Instead bath the infant near to the water source or fill and empty the bath using a jug or similar, smaller volume container.
- If the bath must be moved when full, move using a trolley of a suitable height.
- Beware of water on the floor causing staff/parents to slip.
- Ensure the surface is stable that the bath will be placed on. Brakes must be applied if the trolley/cot is on wheels.
- Any monitoring leads that remain attached to the baby during bathing must not be attached to the monitoring equipment, for reasons of electrical safety.
6.9 Parents
- Parents should be supported and encouraged to be involved in their baby’s bathing whilst on the Unit.
- The special nature of newborn and preterm infants’ skin should be explained to parents, including the rationale behind the skin care aspects of this guideline.
- The frequency and timing of bathing should be negotiated with a baby’s parents to try and balance the parent’s wishes with the baby’s behavioural cues, hygiene needs and skin integrity. However, daily bathing should be discouraged to optimise skin integrity.
6.10 Swaddled Bathing
- Swaddle bathing is the concept of swaddling infants during bathing to reduce stress.
- Nursing observations identify benefits over ‘traditional bathing’ including improved physiological stability, less stress responses, thus reducing energy expended by the baby, and a more pleasurable experience for baby and carer. (Hall, 2008) These observations have not yet been confirmed by research.
- There are different techniques described in the literature, with the basic concept being that the infant is swaddled in a clean cloth before being placed in the water. The infant then either;
- Remains swaddled and flexed during the bath, with individual limbs being exposed and washed in turn, and the back being washed through the cloth. The cloth is only removed before the infant is taken out of the bath.
- The cloth around the infant is gradually released as the baby adjusts to the water and lack of clothes and boundaries. The baby can then enjoy stretching and floating with support from carer.
- Staff should consider this technique for all preterm infants and any vulnerable infants on the Unit, as an alternative to the traditional bathing method commonly used.
- Refer to the Network Guideline ‘Cue Based Cares’ Guidelines: Cue based cares – Neonatal Network South East
6.20 Additional Bathing References
Furdon.S (2003) Challenges in Neonatal Nursing: Providing evidenced based skin care. Highlights of the National Association of Neonatal Nurses (NANN) annual conference 2003. www.medscape.com/viewarticle/465017
Frank.L and D Ouinn (2000) Effect of less bathing of preterm infants on skin flora and pathogen colonization. JOGNN, Vol 28, No?, pp584-89.
Hall.K (2008) Practising developmentally supportive care during infant bathing: reducing stress through swaddle bathing. Infant Vol 4, No 6, pp198-201.
Jackson.A (2008) Time to review newborn skincare Infant Vol 4, No 5, pp168-71.
KEMH (2021) Neonatal Skin Care Guidelines. V2 Women and Newborn Health Care Service King Edward Memorial Hospital. Perth, Western Australia.
Lund. C and Kuller.J (1999) Neonatal skin care: The scientific basis for practice JOGNN, Vol 28, No 3, pp241-54.
Medves.J (2001) Does bathing newborns remove potentially harmful pathogens from the skin? Birth. Vol 28, No 3, pp161-65.
New K (2019) Evidence-based guidelines for infant bathing Research review.co.nz
Raeside.L (2022) Bathing newborn infants. NHSGGC Guidelines, Found at; https://www.clinicalguidelines.scot.nhs.uk/nhsggc-guidelines/nhsggc-guidelines/neonatology/bathing-newborn-infants/
Steen.M (2008) A review of baby skin care Midwives on line- Aug /Sept 2008, www.rcm.org.uk/magazines/papers/a-review-of-baby-skin-care/
Toaland.U (2013) Neonatal Skin Care Guideline. Southern Health and Social Care Trust.
Trotter.S (2004) Care of the Newborn: Proposed new guidelines. British Journal of Midwifery, Vol 12, No 3, pp152-7.
Trotter,S (2004) Neonatal skin care, British Journal of Midwifery, Vol 12, No 5, pp152-7
Xing, S. and Xu, J. et al (2023) Effectiveness of different bathing methods on physiological indexes and behavioural status of preterm infants: a systemic review and meta-analysis. BMC Pediatrics, Vol 23, No 507. Pp1- 12.
Version Control
| Version | Date | Details | Author(s) | Comments |
| 1 | May ‘12 | Final | KR-TVNQCG | TV&W Neonatal Board Approved |
| 2 | Feb ‘16 | Reviewed | KR-TVNQCG | Approved |
| 3 | Feb 2019 | Reviewed and updated | TVWNQCG | Ratified by governance 4.12.2019 |
| 4 | Sept 2024 / Dec 2024 | Reviewed and updated | TVW Guidelines Group | Ratified by governance 12.12.2024 |
| Review Date: | December 2027 | |||
Document version
Version 4
Lead Authors
Thames Valley & Wessex Neonatal ODN Guidelines Group
Approved by
Thames Valley & Wessex Neonatal ODN Governance Group
Approved on
12 December 2024
Renew date
December 2027
Full guide
Related documents
References
Ashford St Peters (2023) Neonatal skin care guidelines, Found at; https://ashfordstpeters.net/Guidelines_Neonatal/Skin%20Care%20Guideline%20Jun%202023.pdf
Atherton.D.J, Genney A.R, Cant.A.J (2004) Rook’s textbook of Dermatology, Vol 1, 7th Ed. Chapter 14: The Neonate. Wiley-Blackwell, Oxford.
Bond.C (2007) Oil for the Neonatal Unit, cherrybond1@aol.com
Bond.C (2009) Baby massage oils, May 2007 cherrybond1@aol.com
Broom M et al (2019) Predicting Neonatal skin injury: The first step to Reducing skin Injuries in Neonates Health Service Insights V12.Pulished online June 14th 2019. Found at; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6572893/
Clemison J and McGuire W (2021) Topical emollient for preventing infection in preterm infants (review) Cochrane Library, Cochrane Database of Systematic Reviews, 2021 Issues 4. No CD001150
DeMeza. T (2013) Should we use olive oil or sunflower oil on a preterm infant’s skin? Infant. Vol 9, No 5, pp170-2
EOE (reviewed 2021) Clinical Guideline: Maintenance of Skin Integrity V1. East of England Neonatal Benchmarking Group.
Gupta P, Nagesh K et al (2023) Evidence based Consensus Recommendations for skin care in Healthy Full Term Neonates in India Pediatric Health Med Ther : 14: 249-265
Jackson, A (2008) Time to review Newborn skin care. Infant Vol 4 (5) 168-71
Kaur S and Sidhu N (2021) Evidence based skin care in Preterm Neonates. Review Article International Journal of Research and Review Vol 8 : Issue 7
Kennedy. R (2020) Clinical Guidelines (nursing) Neonatal and infant Skin care, The Royal Children’s Hospital. Melbourne. www.rch.org.au
KEMH (2021) Neonatal Skin Care Guidelines. Women and Newborn Health Care Service King Edward memorial Hospital. Perth, Western Australia.
Khalfian S et al (2017) Skin care practices in Newborn Nurseries. Perinatol:37 (6):615-621
Kusari.A et al (2019) Evidence based skin care in preterm infants. Pediatric Dermatology, No 36, pp16-23.
Lund.C, and Kuller. J (1999) Neonatal skin care: the scientific basis for practice. Journal of Obstetric, Gynecologic and Neonatal Nursing Vol 28 (3) 241-54
McManus, K. (2016) Infant skin care products: What are the issues . Clinical issues in Neonatal care. Advances in Neonatal care Vol 39 no 55, pp3-12.
Marrisen J, Gomez De Aguero M, et al (2023) The Delicate skin of Preterm infants : Barrier Function, Immune-Microbiome Interaction and Clinical Implications. Neonatology 120(3), pp295-307
Mount Sinai (2023) Skin findings in newborns. Newborn skin characteristics. Found at: https://www.mountsinai.org/health-library/special-topic/skin-findings-in-newborns
OBSeRvE (2015) OBSeRvE: (Oil in Baby Skincare) Study. University of Manchester. Vol 1, Issue 1, p1-4.
Oster, C (2000) Neonatal skin care, the scientific basis for practice. Neonatal Network Vol 19 (1) 49-50
Reed.K (2009) Photographs of correct and incorrect remove of transparent film dressing from skin. Neonatal Unit, John Radcliffe Hospital. Oxford.
Schachner L et al (2021) The importance of skin care for neonates and infants: An Algorithm Journal of Drugs in Dermatoology V 20 Issue 11
Starship (2020) Extremely low birth weight skin care management. Starship.org.nz Guidelines
Taquino.LT (2000) promoting wound healing in the neonatal setting: process versus protocol. Journal of perinatal and neonatal nursing. Vol 14, No 1, June, pp104-118.
Telofski.L et al (2012) The Infant Skin Barrier: Can we preserve, Protect and Enhance the Barrier? Dermatology Research and Practice. Article id 198789, 18 pages.
TVWNODN (2023) Cue Based Care Guideline. Including Swaddled Bathing Parent’s Leaflet. Found at; https://neonatalnetworkssoutheast.nhs.uk/professionals/guidelines/tvw-guidelines/cue-based-cares/
Voegell.D (2008) LBF’ no sting barrier wipes: skin care using advanced silicone technology. British Journal of Nursing, Vol 17, No 7.
Wilbur, W. Amin, R. and Koltner,J et al (2023) Skin care in Infants: A scoping review. Skin Pharmacol Physiol 36 (2) : pp51-56.
Williams.N and Kaiser.A (2012) Does evidence suggest that the use of barrier enhancing emollient is beneficial in the care of preterm neonates. Infant. Vol 8, issue 4, pp120-125.
Implications of race, equality & other diversity duties for this document
This guideline must be implemented fairly and without prejudice whether on the grounds of race, gender, sexual orientation or religion.