
Transfers Section
The information on this page is intended for health professionals reference and use only. If you are a parent or family member looking for information about treatment, please visit unit information.
Contents
1.0 Aim of Guideline
2.0 Scope of Guideline
3.0 Definitions
4.0 Guideline Framework
5.0 Appendices
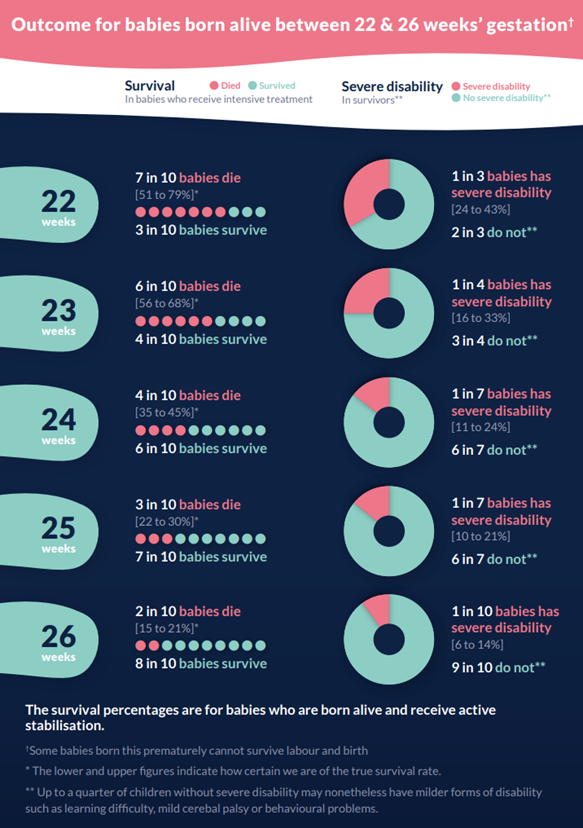
Appendix 1 – Outcome of extreme preterm births infographic
Appendix 2 – BAPM Neonatal Airway Safety Standard. A Framework for Practice (2024) – appendix D
Appendix 3 – Minimum equipment for newborn resuscitation in the pre-hospital environment. Resuscitation Council UK, 2023
Appendix 4 – Neonatal Care Pathway
Appendix 5 – Transfer Care Pathway
Appendix 6 – Communication SBAR for neonatal clinical advice
Appendix 7 – Transfer destination for unwell newborn infants <24 hours of age
Version control and working group contacts
1.0 Aim of Guideline
Framework for Practice
Collaboration between various stakeholders within the Thames Valley & Wessex Neonatal ODN, South Central Ambulance Service SCAS, South West Ambulance Service SWAST, Health Innovation Network Oxford & Thames Valley & Wessex, HEMS, SONeT (Southampton Oxford Neonatal Transport Team), Regional LMNSs and Kent Surrey and Sussex Neonatal ODN. This framework has been developed in accordance with national guidance and standards ie BAPM frameworks, Resuscitation Guidance UK (NLS Guidance and out of hospital recommendations OH NLS.
Task and finish group to support the implementation of the following:
Implement national recommendations for prehospital management of neonates born in an out of hospital setting
- Standardise resource materials for ambulance staff, paramedics, specialist paramedic & emergency care teams and critical care teams within ambulance services
- Develop guidance & recommendations for neonatal care for JRCALC
- Establish remote support advice lines for neonatal prehospital births to support emergency clinicians providing neonatal care
- Establish standardised neonatal care equipment lists for emergency teams
- Establish transfer pathways into hospital neonatal care in accordance with neonatal network pathways
- Standardised education & resource training package for staff for front line staff, sharing of resources to support resuscitation and stabilisation in the prehospital setting
2.0 Scope of Guidelines
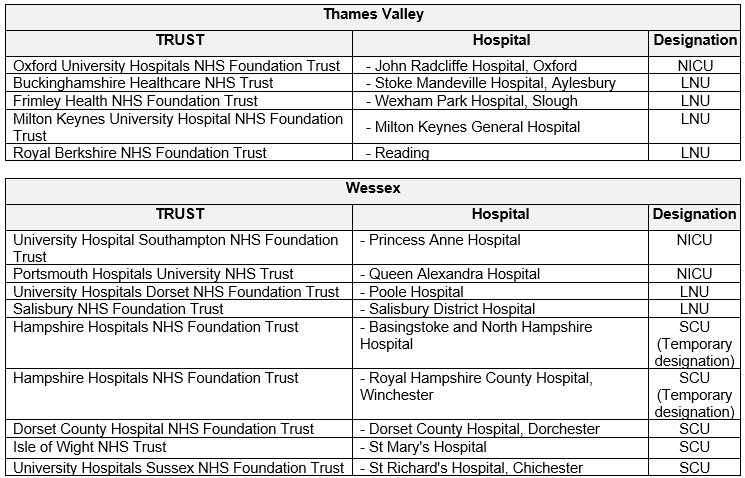
The guideline applies to all neonates who are born in an out of hospital setting including home deliveries and births in an MLU within the SE and SW Region covered by Thames Valley & Wessex Neonatal ODN care pathways. This includes the following destination hospitals: This may extend to other areas covered by prehospital providers ie SWAST, SECAMB within the SE & SW Region.

3.0 Definitions
TVW Thames Valley & Wessex Neonatal ODN
SCAS South Central Ambulance service
SWAST South West Ambulance Service Trust
SECAMB South East Coast Ambulance Service
HEMS Helicopter Emergency Medical Services
SONeT Southampton Oxford Neonatal Transport Team
KSS Kent Surry Sussex Neonatal ODN
BAPM British Association of Perinatal Medicine
JRCALC Joint Royal Colleges Ambulance Liaison Committee
NLS Newborn Life Support
NICU Neonatal Intensive Care Unit
LNU Local Neonatal Unit
SCU Special Care Unit
LMNS Local Maternity and Neonatal System
W3W What 3 Words
OH Out of hospital
4.0 Guideline Framework
NLS (Newborn Life Support) guideline 2021:
Figure 1: Newborn life support algorithm 2021

Extreme preterm babies <27 weeks gestation
These recommendations are based on current national guidance (Pre-hospital management of babies born extremely preterm – a framework for practice. BAPM, 2022) and should be used together to guide clinicians in the care of babies born at less than 27 weeks gestation in the pre-hospital environment.
- Initial assessment of situation:
- Awareness of potential complications during labour and birth that might compromise outcome for either mother or baby
- Determine the gestation of the baby
- Request additional support if birth is imminent
- Prepare an area for resuscitation, off the floor if possible, and open your maternity pack and newborn resuscitation equipment
- For extreme preterm birth, a preterm mask, a food-grade (or neonatal specific) plastic bag and a heated mattress should be available
- Initial management
- Provide effective and timely delivery of appropriate interventions in the mother and baby’s best interests
- Comfort focussed care or attempted stabilisation of the baby based on gestational age (see figure 2: Visual Summary)
- There may not be time to counsel families before the baby is born. The BAPM framework for practice (Perinatal Management of Extreme Preterm Birth Before 27 weeks of Gestation, 2019) may be helpful alongside the outcome of births infographic (appendix 1)
- Correct destination
- Access the most appropriate neonatal and/or maternal expertise at the most appropriate location
- Prioritisation of on-site maternity and neonatal/paediatric facilities may involve bypassing a closer facility. This decision should be made in discussion between the neonatal Consultant and the treating clinicians and should not delay care provision
- Wherever possible, the mother and baby should be transferred to the same hospital
- Pre-alert the hospital
- Communication
- An extremely preterm birth will be a frightening time for both the parents and the attending professionals.
- The language used at this highly emotional time will carry lasting memories for the parents.
- Neonatal clinical advice can be sought from the neonatal transport Consultant (see SBAR structure, appendix 6). This can include advice on clinical care provision, location of care transfer or in situations where resuscitation is futile or unsuccessful.
- In the rare event that an advance care directive or equivalent is in place, this should be confirmed with the parents and respected. This information may be held either in paper or electronic form. A CAD (computer aided dispatch) marker may be added to a home address by the ambulance service.
Active resuscitation (survival focussed care) is not recommended before 22+0 weeks gestation. There should be a focus on comfort-based care.
Comfort-focussed (palliative) neonatal care for the baby and their family will provide families with much comfort in the days and weeks following their baby’s death.
- Parents should be made aware that their baby may show signs of life after birth, including visible heartbeat, gasping and/or movement of limbs.
- The parents should be given time together with their baby, with or without other family members as per their wishes and facilitated to be actively involved in their baby’s care. This should include holding the baby, either skin to skin or swaddled, depending on their preference, and other memory making.
- Remember to offer the parents an opportunity to take photographs.
- If a midwife is in attendance and the mother is stable, the family may prefer to remain at home, otherwise mother and baby should be transported together to maternity care as soon as it is safe to do so.
Survival focused care:
From 22+0 weeks’ gestation, or if gestation is not known, simple interventions focussed on maintaining body temperature and supporting the airway and breathing should be undertaken. This is a time-critical emergency for the baby.
- Thermal care:
- Hypothermia is associated with a poor outcome
- Deferred cord clamping is recommended. Unless there is significant maternal haemorrhage and/or the mother requires urgent medical attention, do not clamp the umbilical cord until 60 seconds have elapsed since birth. Use this time to focus on placing the baby into the polythene bag up to the neck, applying a hat and wrapping with a warm towel/blanket.
- Do not cover the baby’s face.
- Place the swaddled baby on a heated mattress.
- The baby should not be dried unless there is delay in locating a polythene bag. If no bag is available, dry the baby very gently and wrap in a warm towel.
- When the baby has already been dried, a polythene bag will be of less benefit is still recommended.
- Where possible, monitor axilla temperature of the baby. Continuous monitoring may be helpful but care should be taken to ensure the probe is not resting on the heated mattress if one is used.
- Stabilisation and resuscitation as per NLS guidance (see figure 1)
- Maintain thermal care during resuscitation
- Assess the baby and support respiration as per current NLS guidance
- Guidance for neonatal airway equipment and initial respiratory support settings (BAPM 2024) can be found in appendix 2
- Continue airway/breathing support in air (if required) until arrival at destination unless the heartbeat is persistently undetectable
- A saturation probe on the right hand/wrist (preductal) can be helpful to guide oxygen use. Cover the saturation probe with a probe wrap (if available) or towel.
- Transfer to definitive care
- Optimise ambulance temperature and minimise draughts
- Continue providing respiratory support if required
- Ensure that the baby is secured safely for transfer with a flat service available for resuscitation ie. secured to an ambulance stretcher. If available, a vacuum mattress or other commercially available device should be used. Wherever possible, babies should not be transferred in arms.
- Place an early pre-alert to the agreed destination
- Refer to appendices 4 (Neonatal Care Pathway) and 5 (Transfer Care Pathway) to aid decision making and agree the most appropriate destination for the baby
- Neonatal clinical advice can be sought from the neonatal transport Consultant (see SBAR structure, appendix 6). This can include advice on clinical care provision, location of care transfer or in situations where resuscitation is futile or unsuccessful.
- Baby does not appear to respond to resuscitation (BAPM, 2022)
- Where no heartbeat is detectable with a stethoscope on at least two occasions 10 minutes apart and arrival at the destination is not imminent, it is reasonable to reconsider attempts to resuscitate the baby if parents are in agreement with reorientation of care.
- Otherwise continue with ventilation breaths at a rate of 30 breaths per minute until arrival at destination where a decision can be made by the receiving medical team on the appropriateness of continued support.
- Neonatal clinical advice can be sought from the neonatal transport Consultant (see SBAR structure, appendix 6).
Figure 2: Visual summary BAPM Framework of Practise Feb 2022

Preterm babies 27-36+6 weeks gestation
These recommendations follow the same principles as the current national guidance for babies born at earlier gestations (Pre-hospital management of babies born extremely preterm – a framework for practice. BAPM, 2022)
- Initial assessment of situation:
- Awareness of potential complications during labour and birth that might compromise outcome for either mother or baby
- Determine the gestation of the baby
- Request additional support if birth is imminent
- Prepare an area for resuscitation, off the floor if possible, and open your maternity pack and newborn resuscitation equipment. An appropriate size face mask, a food-grade (or neonatal specific) plastic bag and a heated mattress should be available
- Initial management
- Provide effective and timely delivery of appropriate interventions in the mother and baby’s best interests.
- There may not be time to counsel families before the baby is born.
- Correct destination
- Access the most appropriate neonatal and/or maternal expertise at the most appropriate location.
- Prioritisation of on-site maternity and neonatal/paediatric facilities may involve bypassing a closer facility. This decision should be made in discussion between the neonatal Consultant and the treating clinicians and should not delay care provision.
- Wherever possible, the mother and baby should be transferred to the same hospital
- Place an early pre-alert to the agreed destination
- Communication
- Any preterm birth will be a frightening time for both the parents and the attending professionals.
- The language used at this highly emotional time will carry lasting memories for the parents.
- Neonatal clinical advice can be sought from the neonatal transport Consultant (see SBAR structure, appendix 6). This can include advice on clinical care provision, location of care transfer or in situations where resuscitation is futile or unsuccessful.
- In the rare event that an advance care directive or equivalent is in place, this should be confirmed with the parents and respected. This information may be held either in paper or electronic form. A CAD (computer aided dispatch) marker may be added to a home address by the ambulance service.
Simple interventions focussed on maintaining body temperature and supporting the airway and breathing should be undertaken. This is a time-critical emergency for the baby.
- Thermal care:
- Hypothermia is associated with a poor outcome
- Deferred cord clamping is recommended. Unless there is significant maternal haemorrhage and/or the mother requires urgent medical attention, do not clamp the umbilical cord until 60 seconds have elapsed since birth. For babies less than 32 weeks, use this time to focus on placing the baby into the polythene bag up to the neck, applying a hat and wrapping with a warm towel/blanket.
- Do not cover the baby’s face.
- Place the swaddled baby on a heated mattress.
- Babies less than 32 weeks should not be dried unless there is delay in locating a polythene bag. If no bag is available, dry the baby very gently and wrap in a warm towel.
- When the baby has already been dried, a polythene bag will be of less benefit is still recommended
- Where possible, monitor axilla temperature of the baby. Continuous monitoring may be helpful but care should be taken to ensure the probe is not resting on the heated mattress if one is used.
- Stabilisation and resuscitation as per NLS guidance (see figure 1)
- Maintain thermal care during resuscitation
- Assess the baby and support respiration as per current NLS guidance
- Guidance for neonatal airway equipment and initial respiratory support settings (BAPM 2023 – draft framework) can be found in appendix 2
- Continue airway/breathing support in air until arrival at destination unless the heartbeat is persistently undetectable
- A saturation probe on the right hand/wrist (preductal) can be helpful to guide oxygen use. Cover the saturation probe with a probe wrap (if available) or towel.
- Transfer to definitive care
- Optimise ambulance temperature and minimise draughts
- Continue providing respiratory support if required
- Ensure that the baby is secured safely for transfer with a flat service available for resuscitation ie. secured to an ambulance stretcher. If available, a vacuum mattress or other commercially available device should be used. Wherever possible, babies should not be transferred in arms.
- Place an early pre-alert to the agreed destination
- Refer to appendices 4 (Neonatal Care Pathway) and 5 (Transfer Care Pathway) to aid decision making and agree the most appropriate destination for the baby
- Neonatal clinical advice during transfer can be obtained from the neonatal transport Consultant (see SBAR structure, appendix 6). This can include advice on clinical care provision, location of care transfer or in situations where resuscitation is futile or unsuccessful.
Term babies >37 weeks gestation
These recommendations follow the principles of neonatal resuscitation as described in the Newborn Life Support (NLS) guidance (RCUK 2021)
- Initial assessment of situation:
- Awareness of potential complications during labour and birth that might compromise outcome for either mother or baby
- Prepare an area for resuscitation, off the floor if possible, and open your maternity pack and newborn resuscitation equipment.
- Initial management
- Provide effective and timely delivery of appropriate interventions in the mother and baby’s best interests.
- Detailed guidance is available from the Resuscitation Council UK (Newborn resuscitation and support of transition of infants at birth Guidelines, 2021)
- Correct destination
- Transfer may not be required, unless for maternal or baby clinical reasons
- Prioritisation of on-site maternity and neonatal/paediatric facilities may involve bypassing a closer facility if ongoing resuscitation is required (Red Pathway, Appendices 4 and 5). This decision should be made in discussion between the neonatal Consultant and the treating clinicians and should not delay care provision. and should not delay care provision
- Wherever possible, the mother and baby should be transferred to the same hospital
- Pre-alert the hospital if transfer is required
- Communication
- Neonatal clinical advice can be sought from the neonatal transport Consultant (see SBAR structure, appendix 6). This can include advice on clinical care provision, location of care transfer or in situations where resuscitation is futile or unsuccessful.
- In the rare event that an advance care directive or equivalent is in place, this should be confirmed with the parents and respected. This information may be held either in paper or electronic form. A CAD (computer aided dispatch) marker may be added to a home address by the ambulance service.
- Thermal care:
- Hypothermia is associated with a poor outcome
- Deferred cord clamping is recommended. Unless there is significant maternal haemorrhage and/or the mother requires urgent medical attention, do not clamp the umbilical cord until 60 seconds have elapsed since birth
- Dry the infant immediately after delivery.
- Cover the head and body of the infant with a warm towel.
- If no resuscitation is required place the infant skin-to-skin with mother and cover both with a towel. Monitor to ensure continued normothermia.
- If the infant needs support with transition or when resuscitation is required, place the infant on a flat surface, ideally off the floor and away from draughts
- Consider use of a thermal mattress or a polythene bag for maintenance of normothermia and during transfer
- Stabilisation and resuscitation as per NLS guidance (see figure 1)
- Maintain thermal care during resuscitation
- Assess the baby and support respiration as per current NLS guidance
- Guidance for neonatal airway equipment and initial respiratory support settings (BAPM 2023 – draft framework) can be found in appendix 2
- Detailed guidance is available from the Resuscitation Council UK (Newborn resuscitation and support of transition of infants at birth Guidelines, 2021)
- A saturation probe on the right hand/wrist (preductal) can be helpful to guide oxygen use. Cover the saturation probe with a probe wrap (if available) or towel.
- Transfer to definitive care (f required)
- Optimise ambulance temperature and minimise draughts
- Continue providing respiratory support if required
- Ensure that the baby is secured safely for transfer with a flat service available for resuscitation ie. secured to an ambulance stretcher. If available, a vacuum mattress or other commercially available device should be used. Wherever possible, babies should not be transferred in arms.
- Place an early pre-alert to the agreed destination Refer to appendices 4 (Neonatal Care Pathway) and 5 (Transfer Care Pathway) to aid decision making and agree the most appropriate destination for the baby
- Neonatal clinical advice can be sought from the neonatal transport Consultant (see SBAR structure, appendix 6). This can include advice on clinical care provision, location of care transfer or in situations where resuscitation is futile or unsuccessful.
Minimum equipment for newborn resuscitation in the pre-hospital environment:
Resuscitation Council UK guidance for the minimum equipment required in the pre-hospital setting (2023) is based on the core principles of thermoregulation and airway management and can be found in appendix 3.

5.0 Appendices
Appendix 1: Outcome of extreme preterm births infographic
Produced by BAPM alongside the Perinatal Management of Extreme Preterm Birth Before 27 weeks of Gestation. A framework for practice (BAPM, 2019)
Appendix 2: BAPM Neonatal Airway Safety Standard. A Framework for Practice (2024) – appendix D

This guide highlights airway equipment sizes that may be useful to appropriately trained staff and may not be applicable to all staff and situations.
Appendix 3: Minimum equipment for newborn resuscitation in the pre-hospital environment. Resuscitation Council UK, 2023

Appendix 4: Neonatal Care Pathway
Appendix 5: Transfer Care Pathway
Appendix 6: Communication SBAR for neonatal clinical advice
Call
SONeT (Thames Valley and Wessex) 01865 223344
KSS neonatal transport service (KSS) 0207 407 4999
For babies who are anticipated to follow the amber/red pathway, a call for advice pre-delivery may be helpful (if time allows).
Trigger for bypass:
“This is a Direct to Neonatal Consultant call for a pre-hospital newborn on the amber/red pathway. This is an emergency and takes priority over other calls”
Note for hub staff: this call is for clinical advice only and does not need a job number generating. The call should be put through to the transport Consultant immediately. Unless requested by the transport Consultant, the rest of the team do not need to be included in the call.
Communication Structure:
Situation
- Prehospital clinician name, contact details
- “I am calling about a pre-hospital newborn on the amber/red pathway due to …”
- Gestation, age in minutes
- Location
Background:
- Known maternal/newborn comorbidity
- Important events preceding birth
Assessment (currently):
- Airway: Own, iGel, ETT (size)
- Breathing: Supported (continuous, intermittent, PEEP), SpO2
- Circulation: HR, colour, lines, CPR
- Disability: Tone, blood sugar
- Temperature
Response:
- Treatment to date
- Intended transfer location based on geography/table
Appendix 7: Transfer destination for unwell newborn infants <24 hours of age
Version control
| Version | Date | Details | Author(s) | Comments |
| 1 | March 2024 | Pre-hospital management task and finish working group 2022/ 2023
|
VP, JW and Pre-hospital management task and finish working group | Draft circulated May 2024 to:
Pre-hospital management task and finish working group, KSS ODN team (Clinical lead, Manager and Nurse Lead), LMNS Patient Safety Leads and LMNS SROs / Project Officers, TVW Guidelines Group, TVW Medical and Nurse Leads, TVW Practice Educators, TVW ANNPs and TVW Pharmacists. |
| 2 | Sept 2024 | Edits following circulation | VP, JW and Pre-hospital management task and finish working group | Comment received and incorporated from:
Matt Taylor (UHD) Hannah Leonard (NHS Dorset) James Yates (SWAST) Craig Wilkins (SWAST) Philip Amess (Sussex LMNS) Hannah Mallon (UHS) John Black (SCAS) Dawn Kerslake (SECAmb) |
| Review Date: | September 2027 | |||
Pre-hospital Management of the Preterm Infant working group members:
Aung Soe, KSS Neonatal ODN Clinical Lead
Craig Wilkins, SWAST
Dan Cody, SECAMB
Darren Best, SCAS
Dawn Kerslake, Consultant Midwife SECAMB
Debbie Gray, SCAS
Eileen Dudley, BOB LMNS and Health Innovation Oxford
Eleri Adams SONET Lead
Fionna Moore, SECAMB
Gina Outram, TVW Neonatal ODN Manager
Jennifer Lomas, KSS Neonatal ODN Manger
Jenny Weddell, UHS SONeT Nurse Lead, University Hospital Southampton NHS FT
John Black, CMO SCAS
Kate Graham-Evans, Neonatologist Portsmouth Hospitals University NHS Trust
Kirsten Willis Drewett, SCAS
Kirsten McGilligan MLU Banbury
Lambri Yianni, Consultant Neonatologist University Hospital Southampton NHS FT
Matt Thomas, Medical Director SWAST
Matthew Taylor, Intensive Care Consultant, HEMS Dorset Philip Cowburn, SWAST
Philip Hyde, PICU University Hospital Southampton NHS FT
Rachel Garrett, Health Innovation Kent Surrey Sussex
Rebecca Black, Oxford University Hospitals NHS FT
Rob Summerhayes. HEMS Consultant and Education lead at HIOWAA (Hampshire and Isle of Wight Air Ambulance
Samantha Fleming, Royal Berkshire NHS FT
Sarah Davidson, UHS SONeT Consultant Lead, University Hospital Southampton NHS FT
Steph Pearce – Education Manager Midwife South Central Ambulance Service
Simon Brown, SCAS
Victoria Puddy, University Hospital Southampton NHS FT and TVW Neonatal ODN
Working groups:
Health Innovation Oxford
Health Innovation Wessex
Health Innovation Kent Surrey Sussex
Document version
Version 2
Lead Authors
Dr Victoria Puddy, TV & Wessex Clinical Lead
Jenny Weddell, UHS Hub SONeT Nurse Lead
Prehospital Management Working Group
Approved by
Thames Valley & Wessex Neonatal ODN Governance Group
Approved on
19th September 2024
Renew date
September 2027
Full guide
Related documents / references
Pre Hospital management of the baby born at extreme preterm gestation. A BAPM Framework for Practice Feb 2022.
https://www.bapm.org/resources/pre-hospital-management-of-the-baby-born-at-extreme-preterm-gestation
Visual Summary: https://hubble-live-assets.s3.amazonaws.com/bapm/file_asset/file/898/Pre-hospital_management_summary_15-02-2022.pdf
NLS resuscitation guidelines 2021 – Resuscitation Council UK
https://www.resus.org.uk/library/2021-resuscitation-guidelines/newborn-resuscitation-and-support-transition-infants-birth
Newborn Life Support Algorithm 2021
https://www.resus.org.uk/sites/default/files/2021-05/Newborn%20Life%20Support%20Algorithm%202021.pdf
Perinatal Management of Extreme Preterm Birth before 27 weeks of gestation A Framework for Practice, BAPM October 2019
https://www.bapm.org/resources/80-perinatal-management-of-extreme-preterm-birth-before-27-weeks-of-gestation-2019
Outcomes of Births Infographic (BAPM)
https://hubble-live-assets.s3.eu-west-1.amazonaws.com/bapm/file_asset/file/31/outcome-of-births-infographic-201909111005-colour.pdf
BAPM Neonatal Airway Safety Standard A Framework for Practice (2024)
https://www.bapm.org/resources/BAPM-Neonatal-Airway-Safety-Standard
Resuscitation Council UK Newborn resuscitation and support of transition of infants at birth Guidelines (May 2021)
https://www.resus.org.uk/library/2021-resuscitation-guidelines/newborn-resuscitation-and-support-transition-infants-birth
Implications of race, equality & other diversity duties for this document
This guideline must be implemented fairly and without prejudice whether on the grounds of race, gender, sexual orientation or religion.